September is PCOS Awareness Month
As a Physician Assistant, female and, endometriosis warrior, I’ve found that women’s health issues are some of my favorite to discuss. Not only are they a part of my own story, but they are also a huge source of empowerment for women. The more we know and understand our bodies, the more we can begin to take control of them.
So let’s start the conversation about PCOS!
PCOS, or Polycystic Ovarian Syndrome, is a hormonal disorder that causes problems in the ovaries. It’s associated with high levels of androgens, also known as “male hormones”, but are also synthesized by females in smaller amounts. The higher level of androgens can cause abnormal hair growth and missed/irregular periods, two common signs of PCOS. Irregular periods can lead to the development of ovarian cysts. Women with PCOS have also been found to have higher occurrence of insulin resistance. Obesity and genetics may play a role in that, but over time if untreated, many women with PCOS may develop type 2 diabetes.

PCOS affects 1 in 10 women of childbearing age. It’s the most common cause for anovulatory infertility and the most common cause of oligomenorrhea (infrequent periods) and amenorrhea (lack of menstruation) worldwide. It’s often diagnosed when a woman is attempting to get pregnant and struggling with infertility. The cause of PCOS is still misunderstood. There is however a genetic predisposition for females who have a mother, sister, or aunt with it.
Common Symptoms of PCOS
The most common symptom of PCOS is metrorrhagia (aka irregular periods). However, just because you have irregular periods does not mean you have PCOS. Some females with PCOS have menorrhagia (or heavy periods), but both irregular and heavy periods are not normal symptoms and should be investigated further by your gynecologist. Other symptoms of PCOS include abnormal hair growth (hirsutism), acne, thinning of the hair, weight gain, darkening of the skin (acanthosis nigricans), and skin tag formation. PCOS is often diagnosed when a female presents with fertility issues. Because the ovaries aren’t ovulating appropriately, this can make it challenging for a women to become pregnant without any treatment.
Tests for PCOS
Unfortunately, there is no definitive test for PCOS. An OB-GYN or medical provider will take a number of considerations into account before diagnosing a patient with PCOS. Some of those considerations include physical exam, BMI, transvaginal ultrasound, pelvic exam, and blood work (androgens, cholesterol, glucose tolerance, triglyceride levels).
Rotterdam Criteria for PCOS
This criteria was created for the diagnosis of PCOS. If a patient has 2 out of the 3 criteria, then the diagnosis can be made. However in clinical practice, other conditions (including thyroid dysfunction, NCCAH, hyperprolactinemia, and androgen-secreting tumors) are often excluded prior to a formal diagnosis. Below are the three criteria:

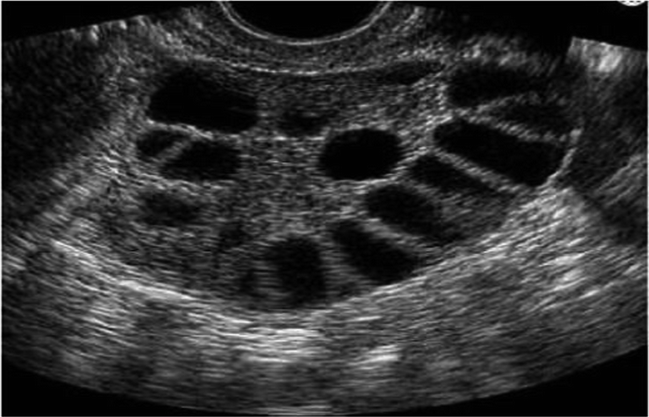
PCOS on Ultrasound
Below are transvaginal ultrasound images of the ovaries. The dark areas are what are called follicles, and each follicle is fluid-filled. If a patient has 12 or more of these follicles in their ovaries, your doctor may consider further testing for PCOS.


Complications of PCOS
- Infertility
- Gestational diabetes
- Miscarriage or premature birth
- Non-alcoholic fatty liver disease
- Metabolic syndrome — a cluster of conditions including high blood pressure, high blood sugar, and abnormal cholesterol or triglyceride levels that significantly increase your risk of cardiovascular disease
- Type 2 diabetes or prediabetes
- Sleep apnea
- Depression, anxiety and eating disorders
- Abnormal uterine bleeding, aka irregular periods
- 3X increased risk of developing Endometrial cancer
Like most medical conditions, if left untreated, PCOS can have severe effects on your mental and physical health. That’s why understanding the signs and symptoms is so important so that your doctor can perform the appropriate testing and get you the right treatment.
Treatment for PCOS
Treatment is individually-based and focused on the patient’s specific symptoms. Unfortunately, there is no cure to PCOS at this time. Oftentimes lifestyle modifications, including weight loss, low-carb diets, and regular exercise, may be recommended to decrease the effects of PCOS. To regulate one’s menstrual cycle or period, combination birth control or progestin-only therapy may be prescribed. To help a patient ovulate, Clomid, Femara, Metformin, or gonadotropins may be prescribed. To help reduce hair growth, Sprionolactone, Vaniqa cream, combination birth control, or electrolysis, may be of benefit.

Clomid (clomiphene citrate or Serophene): an oral anti-estrogen medication taken during the first part of your menstrual cycle to induce ovulation. It works by making your body think your estrogen levels are lower than they are, which causes the pituitary gland to increase secretion of follicle stimulating hormone, or FSH, and luteinizing hormone, or LH. Higher levels of FSH stimulate the ovary to produce an egg follicle, or multiple follicles, that will develop and be released during ovulation. High levels of LH stimulate ovulation. Possible side effects include headache, nausea, vomiting, pelvic pain, abnormal vaginal bleeding, flushing, and breast tenderness.
Femara (letrozole): an aromatase inhibitor that stops the production of estrogen in your body to increase FSH and LH production. In a study performed by the AAFP, Femara was more effective at increasing the chances of pregnancy in subfertile women with PCOS than Clomid. Possible side effects include hot flashes, hair loss, joint/muscle pain, drowsiness, weight gain, and night sweats.
Metformin (glucophage): an ovulation induction agent for non-obese women with PCOS. It reduces insulin levels and alters the effect of insulin on ovarian androgen biosynthesis, theca cell proliferation, and endometrial growth. Possible side effects include nausea, vomiting, abdominal pain, diarrhea, and loss of appetite.
Spironolactone (aldactone): an aldosterone receptor antagonists that works to reduce the production of androgens, which in turn reduces hair growth and improves acne. It is often used in dermatology to target the hormonal causes of acne. Possible side effects include nausea, vomiting, abnormal vaginal bleeding, drowsiness, breast tenderness, and increased hair growth.
Vaniqa: the first and only prescription cream proven to reduce unwanted facial hair. Possible side effects including headache, temporary redness of the skin, and skin dryness.
Diet Changes Recommended for PCOS
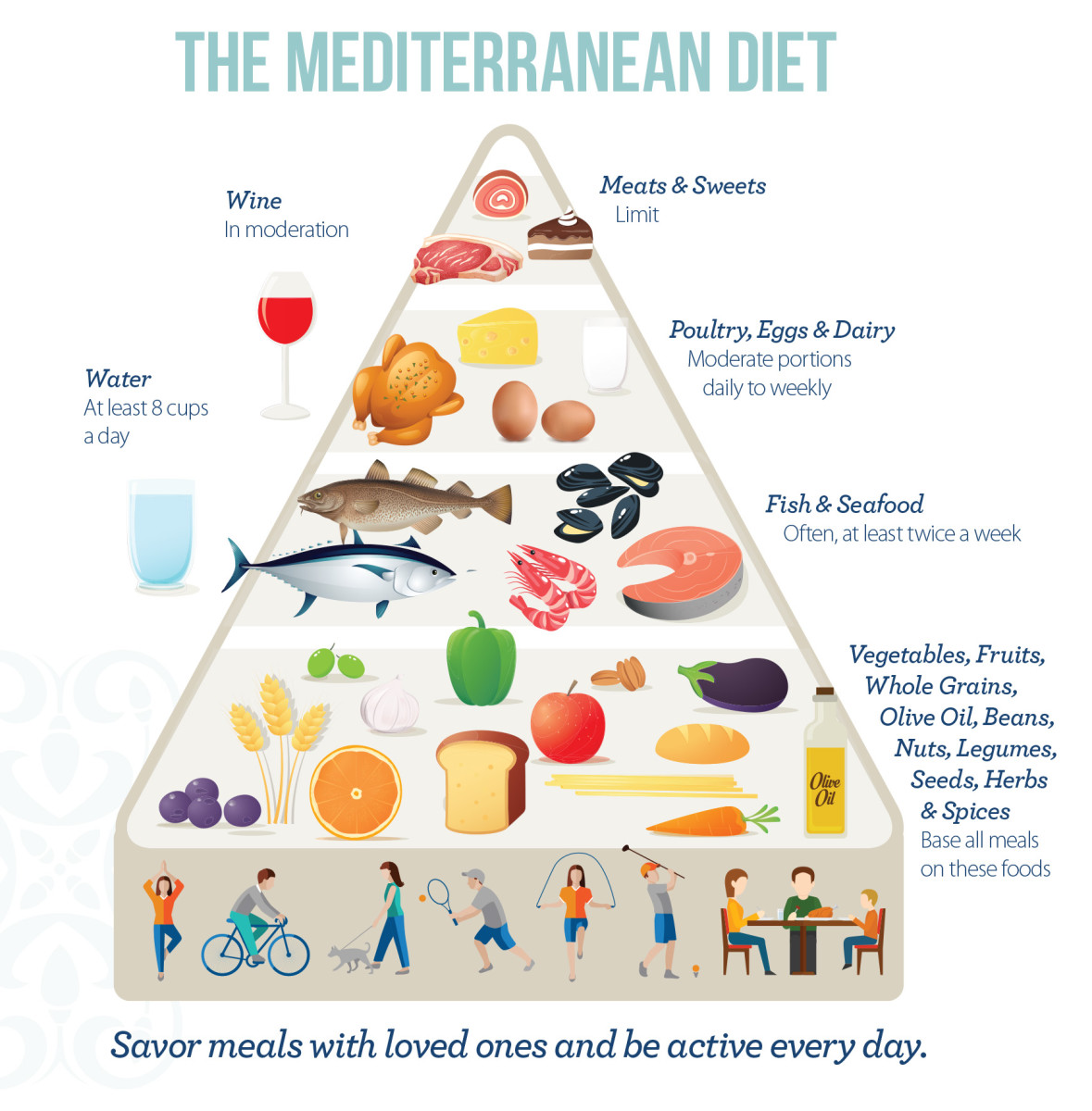
Because PCOS causes insulin resistance, dietary changes should be implemented for holistic therapy. PCOS is characterized by chronic low-grade inflammation, so ways to combat that would include keeping blood sugars in check and maintaining a healthy weight. Diets that are encouraged for individuals with inflammatory states include the Mediterranean diet and the DASH diet. The Mediterranean diet consists of fruits, vegetables, seafood, whole grains, and healthy fats. The DASH diet was originally created for controlling high blood pressure, however it’s been shown to be of benefit for individuals who are managing their insulin levels as well. It focuses on the consumption of fruits, vegetables, whole grains, poultry, fish, legumes, nuts, and seeds. But by incorporating more lean protein, high, fiber, and antioxidant-rich foods, individuals have been found to lessen the severity of some of their PCOS symptoms. Limiting refined carbs, processed foods, saturated/trans fats, dairy, and alcohol can also be of benefit. And if you think about it, these dietary changes are healthy for all individuals, not just those in a chronic inflammatory state.

PCOS Resources
American College of Obstetricians and Gynecologists
American Society for Reproductive Medicine
The Hormone Health Network
PCOS Awareness Association
PCOS Challenge
PCOS PDF – Resources for a Healthier You
Resolve: The National Infertility Association
Talk to Your Doctor
I’ve said this before, and I’ll say it again. If you ever have questions or concerns about your physical health, talk to your doctor. Raise your concerns. Ask questions and be an advocate for your health. Oftentimes as females, we are afraid to ask questions because we are afraid we may sound ignorant. But staying silent is worse than never letting your voice be heard. DO NOT let fear stand in the way of getting answers and treatment.
PCOS affects 1 in 10 women of childbearing age. Do not delay your care and treatment. If you find yourself struggling with infertility or questioning why you have infrequent or periods, it may be time to reach out to your OB-GYN for answers.









Leave a comment