My name is Sarah Brown and I have endometriosis.
In the past, I’ve shared my struggles with receiving this diagnosis. However, this post is a follow-up to shed light on this often misunderstood disorder. There’s been a lot more publicity over the past couple months promoting awareness of the disorder, which I can honestly say I’m thankful for. Given the fact that 1/10 women have endometriosis, this disorder needs to be better understood so that women can pick up on their symptomatology and ask for help accordingly.
What is endometriosis?
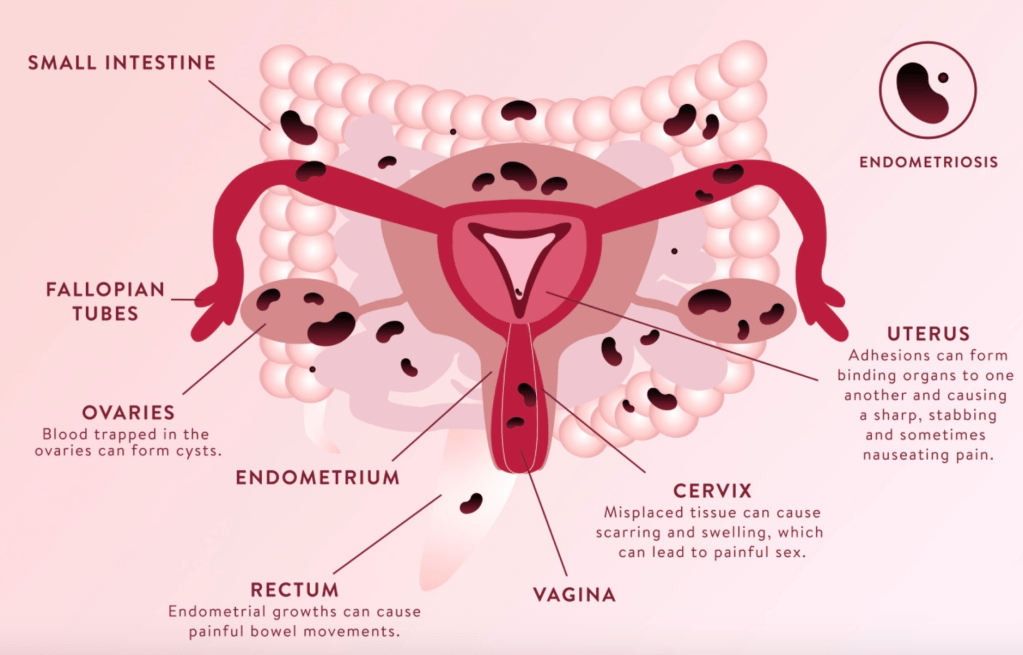
Endometriosis is essentially a disorder where uterine tissue begins to grow outside the uterus. The pathophysiology of why this happens is still unclear at this time. There are a handful of hypotheses floating around about what causes endo, however the most widely known hypothesis relates to retrograde menstruation. In retrograde menstruation, menstrual blood containing endometrial cells flows back through the fallopian tubes into the pelvic cavity. Displaced endometrial cells then begin to stick to the pelvic wall and pelvic organs, where they continue to grow and thicken and bleed over the course of each menstrual cycle. This hypothesis has not yet been proven, but it’s an interesting take on a very misunderstood disease.
Below is an infographic showing the different areas of the pelvic cavity in which endometrial tissue can grow. The most common sites for endo are the ovaries, Fallopian tubes, uterosacral ligaments, the anterior & posterior cul-de-sac, the surface of the uterus, and the lining of the pelvic cavity. However, it can grow into the intestines, rectum, bladder, vagina, cervix, and vulva. In rare cases, endometrial implants have been found in the lungs, brain, and heart.
What are the symptoms of endometriosis?
The most common symptom associated with endometriosis is dysmenorrhea (aka painful periods). This symptom can be difficult to ascertain since periods in nature are painful, however the extent of pain experienced for patients with endometriosis can be quite severe. But let me be clear, just because you have painful periods does not mean that you have endometriosis. Other symptoms experience in endometriosis patients include painful intercourse (dyspareunia), pain with bowel movements, excessive bleeding (menorrhagia), and infertility. FUN FACT: the most common cause of infertility in an otherwise healthy female is often secondary to endometriosis.
How can you get tested for endometriosis?
Here’s the trickiest part: the only definitive way to diagnose this disorder is through a laparoscopy (aka a surgical procedure). Helpful tools that guide the practitioner to suggest a laparoscopy include transvaginal ultrasounds, pelvic exams, and blood work. Unfortunately at this time, the only way to truly know whether there is endometrial tissue outside the uterus is to physically lay eyes on the pelvic cavity which can only be done via a laparoscopy.
It’s not easy being a patient when you’re a healthcare provider, because you often know the ramifications of your diagnosis, treatment, and worst-case -cenario of the disease state. I found that out quickly when I had my laparoscopic abdominal surgery in May of 2018. When you receive troubling news or a hard diagnosis, it’s all too easy to jump to conclusions about what this means for your future.
What are the risk factors?
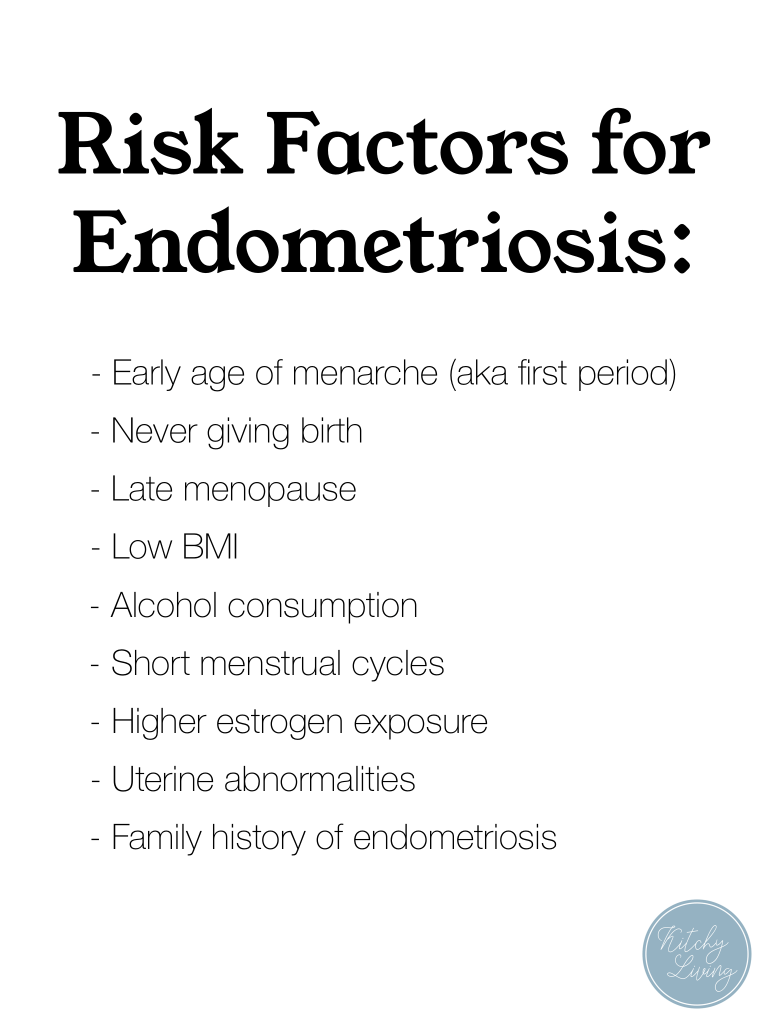
What risks are associated with endometriosis?
The two main risks associated with this disorder are infertility and ovarian cancer. Infertility is often the way that women find out that they have endometriosis. Due to the abnormal tissue growth within the pelvic cavity, it makes implantation of the fertilized egg challenging for endometriosis patients. Just because it’s difficult does not mean that it is impossible though. Endometriosis patients are at higher risk of infertility than the general female population, however only 30-50% of endometriosis patients struggle with fertility with even less actually being infertile after significant time and treatment. Infertility can be a major struggle with these women, so understanding the ramifications and interference this disorder can have on the life of reproductive-age women is huge.
Also, patients who have received the diagnosis of endometriosis via laparoscopy will be tested either prior or after surgery for their ovarian cancer risk. This can be done by a simple blood test (OVA-1 or CA-125). These will provide the patient with a better understanding of their lifetime risk of developing ovarian cancer. In the general population, 1 in 75 women will develop ovarian cancer within their lifetime, which is approximately a 1.33% lifetime risk. Ovarian cancer is a very rare form of cancer, however women with endometriosis should be aware of this risk and get proper testing done.
Is there a cure?
Unfortunately, like many medical disorders, there is no cure for endometriosis. However there are a variety of treatment options hand-tailored to the needs of each patient.
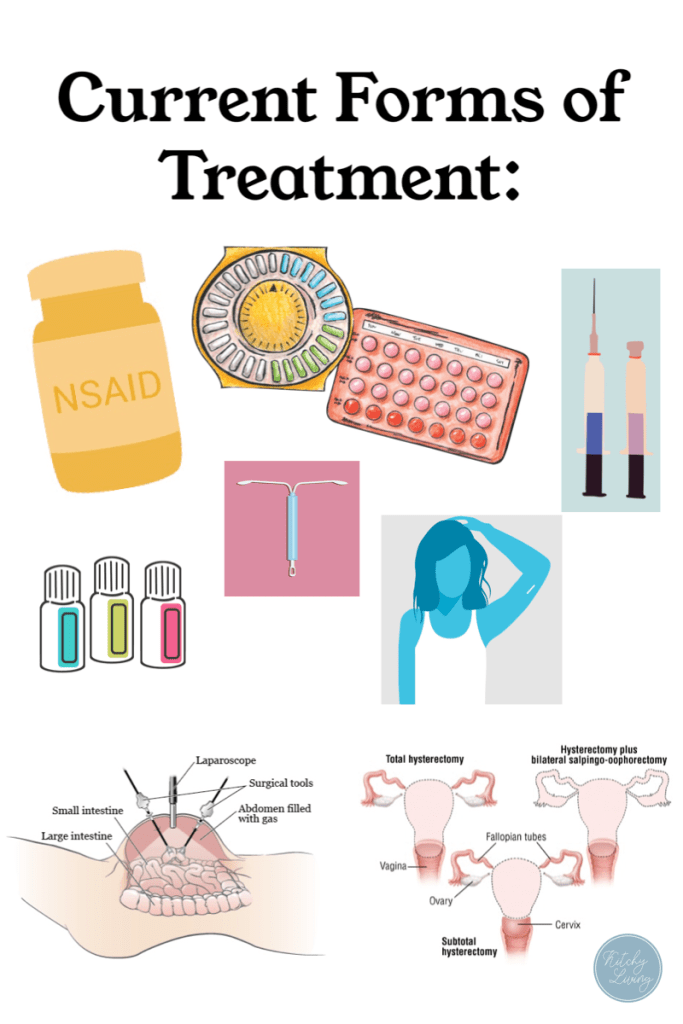
The first form of treatment being painkillers to help with ongoing inflammation and endo-pain. These can be found both over-the-counter or by prescription. Narcotics are not first-line, nor should they really be considered unless a patient is Stage 4 and experiencing excruciating bouts of abdominal pain. NSAIDs are a great option for endometriosis pain and can include ibuprofen (Motrin, Advil) or naproxen sodium (Aleve).
Another treatment option is hormonal birth control. Most endometriosis patients (unless contraindicated) should be on a regular form of hormonal birth control. This helps to reduce estrogen fluctuation and also if packs are taken back to back to back without taking the placebo, this further prevents endometrial tissue from implanting elsewhere within the body because you are not allowing the body to produce/secrete endometrial tissue. Hormonal birth control includes oral contraceptive pills (OCPs), intrauterine devices, Progestin injections (Depo), and Implants (Nexplanon).
Laparoscopy procedures are a great treatment for women who know they have endometriosis and are about to try to get pregnant. The surgery consists of ablation and excision of the endometrial tissue within the pelvic cavity that is causing the severe pain. These procedures are diagnostic and therapeutic in that they are the only way to properly diagnose endometriosis and they therapeutically rid the patient of the unwanted tissues.
Gonadotropin-releasing hormone (GnRH) agonist medications are another more severe form of treatment that is considered more for Stage 3 & 4 patients due to the drastic symptoms and severe risk factors that are associated with their use. Essentially these agonist medications are chemotherapetic agents that have had a long-term use for prostate cancer and precocious puberty. Risks associated with GnRH agonists include bone thinning (osteoporosis) and menopausal-type symptoms (insomnia, decreased libido, vaginal dryness, dizziness, depression, acne, mood swings, headaches). Although add-back therapy is often utilized to reduce these risks, GnRH agonists should not be considered standard care of practice for every endometriosis patient.
Gonadotropin-releasing hormone (GnRH) antagonist medications are similar to the above medication. The main difference is their mechanism of action. They bind competitively to GnRH receptors which prevents the action of endogenous GnRH on the pituitary. It also reduces the body’s levels of estrogen, which is considered one of the main culprits for endometriosis proliferation. Once again, this medication is a consideration for moderate to severe endo patients. An example of this is Orilissa. It’s marketed as a non-hormonal form of treatment that’s been clinically proven to reduce painful periods, pelvic pain in between periods, and pain with sex. Side effects are the same as the above GnRH agonists.
The only true end to endometriosis is by way of a hysterectomy (aka surgical removal of the lady parts). For most women of childbearing age living with endometriosis, a hysterectomy is not first-line treatment due to the fact that they often wanna have babies before taking out their uterus. This surgical procedure is irreversible, therefore if the patient knows they no longer want to have children, this would be the means to which they could get rid of their endometriosis once a for all.
Brief Overview
Osmosis.org created a succinct 9-minute YouTube video hitting the highlights of Endometriosis. I highly recommend watching it to get a more general understanding!
How am I choosing to live with endometriosis?
I can truthfully say that the weeks following my surgery, I scoured the literature for hours and hours each day trying to find healthy, non-pharmacologic alternatives to treating endometriosis. However at this time, many of the non-pharm treatments lack sufficient data and clinical trials to prove their worth. Therefore, I am currently sticking to hormonal birth control by way of oral contraceptives and NSAIDs in combination with the occasional roller blend of essential oils. I’ve read a lot about limiting your dietary estrogen intake to prevent flares from occurring as well, so I try to limit the amount of dairy I eat/drink, try to buy meats without hormones or antibiotics, and try to limit the amount of foods I consume that have estrogen in them (edamame, soy milk, tofu, etc.). I don’t know if any of that makes a bit of difference to my endometrial tissue, but being able to make those little changes to my diet makes me feel as if I’m making an effort to kick this disorder in the butt. Pretty much, I’m choosing to live with endometriosis but not let it define me, as I think many females living with this terrible disorder should do. I didn’t desire to have this be a part of my story, however after May 24, 2018 it has become a chapter of mine whether I like it or not.

I hope that through sharing my story, explaining the physiology, and shedding light on this often misunderstood disorder I have broadened your knowledge and understanding of endometriosis. If you ever have any questions about this disorder or my journey, please feel free to contact me or leave a comment below. Just remember that you are not alone in whatever trials you struggle through, and that God is making all things new minute by minute of every day. Share your story and embrace the vulnerability, because God can use that vulnerability to further his kingdom and spread his love.









Leave a comment