March is Endometriosis Awareness Month
And for those of you that don’t know, I have endometriosis. I was diagnosed with it in May 2018 after having a laparoscopic procedure to remove an ovarian cyst. But when I got the initial diagnosis, I was devastated. In my mind, I thought that it was a death sentence: painful periods, risk of infertility, no cure. But with lots of time and processing, I’ve come to realize it’s not a death sentence. It’s an obstacle, yes. But endometriosis doesn’t have the last word in my story. So if you too have endometriosis, take heart, because this burden we bear makes us stronger.
Also, keep in mind that endometriosis is in stages. So one person’s experience with endo can be vastly different from another person’s experience. Endometriosis looks different and poses different challenges to each individual. So the phrase “comparison is the thief of joy” couldn’t ring truer when talking about this chronic inflammatory disorder.


An unfiltered picture of my abdomen the day of my laparoscopy. I had three incisions: one in my umbilicus and two on my lower abdomen. They are basically non-existent now which is amazing when you think about the healing our bodies are capable of!
So let’s talk Endometriosis!
What are the most common symptoms of Endometriosis?
How do you diagnose Endometriosis?
The only definitive way to diagnose this disorder is through laparoscopy (aka a surgical procedure). Helpful tools that guide the practitioner to suggest a laparoscopy include transvaginal ultrasounds, symptoms, pelvic exams, and blood work. Unfortunately at this time, the only way to truly know whether there is endometrial tissue outside the uterus is to physically lay eyes on the pelvic cavity, which can only be done via a laparoscopy.
Are there risk factors that predispose you to a diagnosis?

What causes Endometriosis?
Unfortunately at this time, the cause of endometriosis is unknown. Multiple theories exist, however each are hypotheses that need further research to be validated. This is why it is so vital for us to invest in increased endometriosis research within the medical community. It is more likely that there is more than one cause for endometriosis, therefore it is useful to understand each theory.
1. Stem Cell Theory
Stem cell theory proposes that the cells responsible for the regeneration of the endometrial lining during one’s menstrual cycle play a role in the development of endometriosis. The spreading of these stem cells to ectopic regions can then lead to the differentiation of endometrial cells and cause endometriosis.
2. Sampson’s Theory of Retrograde Menstruation
One of the oldest theories explaining the etiology of endometriosis, proposes menstrual blood containing endometrial cells flows backward through the fallopian tubes and into the pelvic cavity. These endometrial cells that should have been shed during menstruation then lead to implantation and further spreading of endometriosis lesions.
3. Mulleriosis & Embryonic Origin Theory
The theory of mulleriosis posits that the cause of endometriosis lies in developmental abnormalities in the female reproductive system. It proposes that endometriosis occurs due to abnormal differentiation or migration of any component of the mullerian duct system. This system is a channel in the early embryo that goes on to develop into the fallopian tubes, uterus, and cervix.
4. Genetics
Endometriosis has been studied through a micro perspective in the case of changes in gene expression to a more macro level in terms of what it means to have a family history of endometriosis. With one first-degree family member affected (mother, sister, daughter), a woman has an increased risk of having endometriosis. A family history of endometriosis can increase the risk of earlier age of symptom onset, similar symptoms or more severe symptoms, and infertility.
5. Uterine Peristalsis
Uterine peristalsis, the rhythmic contraction and relaxation of tissue muscle, is one of the fundamental functions of the non-pregnant uterus. Contractions of the uterus allow for proper menstruation and are involved in early reproductive processes, such as sperm transportation and egg implantation. Dysfunctional uterine peristalsis may play a part in the development of endometriosis, particularly through the process of retrograde menstruation.
6. Hormones
Estrogen and progesterone have been a subject of much debate amongst endocrinologists in all sorts of endometriosis theories. More research is needed to fully understand the exact role of estrogen and progesterone in the development of endometriosis.
7. Lymphatic System
The lymphatic system is part of the circulatory system and is responsible for carrying and removing fluids from the body’s tissues. This fluid can contain a variety of essential life components, including red blood cells, white blood cells, and plasma. Many have proposed that this system plays a role in transporting endometrial cells to other parts of the body, which explains how endometriosis can spread throughout the body. The lymphatic system also serves as a connection for endometriosis involvement with the immune system.
8. Immune System
The immune system is responsible for protecting the body from disease. In endometriosis, the affected areas become excessively red and swollen. Because an inflammatory response typically occurs when the body is fighting an infectious disease, the immune system’s role in endometriosis progression has become a subject of much interest. Researchers suspect that an issue in the immune system may make the body ill-equipped to recognize and destroy endometrial tissue growing outside of the uterus.
9. Oxidative Stress
Free radicals are highly reactive molecules of oxygen. Typically, the body will manage these molecules with anti-oxidants. Although some free radicals can be beneficial for the body, an excessive amount can be harmful. The elevation of free radicals in the peritoneum (lining of the abdomen), and lack of anti-oxidants, is suspected to be one of the links in the chain of events causing endometriosis.
10. Apoptosis
Apoptosis occurs when the body signals out dysfunctional cells which could be harmful and destroys them. This is a highly regulated mechanism and is key in the body’s maintenance of preventing disease. In fact, the malfunction in the mechanisms regulating apoptosis is a common cause of cancer. As the body cannot rid itself of harmful, damaging cells, these cells grow and spread, causing tumors and cancer. Endometriosis cells have the capacity to avoid apoptosis. The role this plays in the development of the disease is currently being investigated
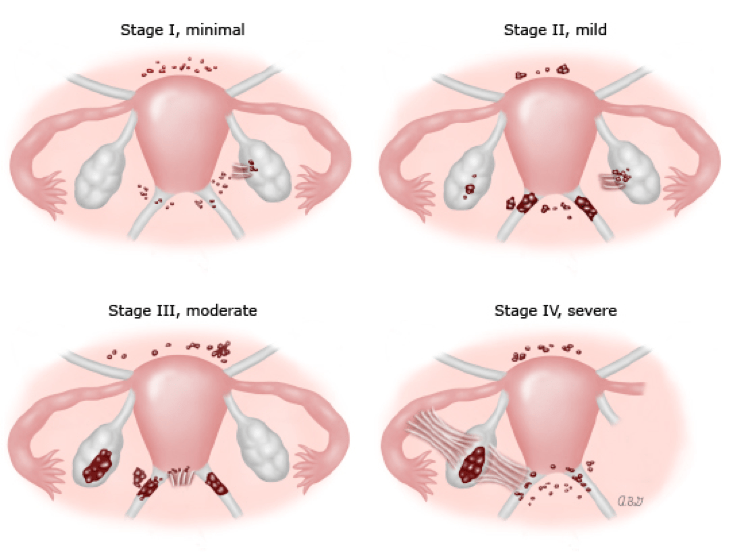
Staging of Endometriosis
To help classify the severity of endometriosis, the American Society of Reproductive Medicine (ASRM) created a staging system as seen below…
Stage I (1-5 points): minimal, few superficial implants
Stage II (6-15 points): mild, more and deeper implants
Stage III (16-40 points): moderate, many deep implants, small cysts on one or both ovaries, presence of filmy adhesions
Stage IV (>40 points): severe, many deep implants, large cysts on one or both ovaries, many dense adhesions
What risks are associated with having endometriosis?
The two main risks associated with this disorder are infertility and ovarian cancer. Infertility is often the way that women find out that they have endometriosis. Due to the abnormal tissue growth within the pelvic cavity, it makes implantation of the fertilized egg challenging for endometriosis patients. Just because it’s difficult does not mean that it is impossible though. Endometriosis patients are at higher risk of infertility than the general female population, however only 30-50% of endometriosis patients struggle with fertility with even less actually being infertile after significant time and treatment. Infertility can be a major struggle with these women, so understanding the ramifications and interference this disorder can have on the life of reproductive-age women is huge.
Also, patients who have received the diagnosis of endometriosis via laparoscopy will be tested either prior or after surgery for their ovarian cancer risk. This can be done by a simple blood test (OVA-1 or CA-125). These will provide the patient with a better understanding of their lifetime risk of developing ovarian cancer. In the general population, 1 in 75 women will develop ovarian cancer within their lifetime, which is approximately a 1.33% lifetime risk. Ovarian cancer is a very rare form of cancer, however women with endometriosis should be aware of this risk and get proper testing done.
What treatment options are available?

The first form of treatment being painkillers to help with ongoing inflammation and endo-pain. These can be found both over-the-counter or by prescription. Narcotics are not first-line, nor should they really be considered. NSAIDs are a great option for endometriosis pain and can include ibuprofen (Motrin, Advil) or naproxen sodium (Aleve).
Another treatment option is hormonal birth control. Most endometriosis patients (unless contraindicated) would benefit from being on a form of hormonal birth control. This helps to reduce estrogen fluctuation and also if oral contraceptive packs are taken back to back-to-back without taking the placebo, this further prevents endometrial tissue from implanting elsewhere within the body because you are not allowing the body to produce/secrete endometrial tissue. Hormonal birth control includes oral contraceptive pills (OCPs), intrauterine devices, Progestin injections (Depo), and Implants (Nexplanon).
Laparoscopy procedures are a great treatment for women who know they have endometriosis and are about to try to get pregnant. The surgery consists of ablation and excision of the endometrial tissue within the pelvic cavity that is causing the severe pain. These procedures are diagnostic and therapeutic in that they are the only way to properly diagnose endometriosis and they therapeutically rid the patient of the unwanted tissues.
Gonadotropin-releasing hormone (GnRH) agonist medications are another more severe form of treatment that is considered more for Stage 3 & 4 patients due to the drastic symptoms and severe risk factors that are associated with their use. Essentially these agonist medications are chemotherapetic agents that have had a long-term use for prostate cancer and precocious puberty. Risks associated with GnRH agonists include bone thinning (osteoporosis) and menopausal-type symptoms (insomnia, decreased libido, vaginal dryness, dizziness, depression, acne, mood swings, headaches). Although add-back therapy is often utilized to reduce these risks, GnRH agonists should not be considered standard care for every endometriosis patient.
Gonadotropin-releasing hormone (GnRH) antagonist medications are similar to the above medication. The main difference is their mechanism of action. They bind competitively to GnRH receptors which prevents the action of endogenous GnRH on the pituitary. It also reduces the body’s levels of estrogen, which is considered one of the main culprits for endometriosis proliferation. Once again, this medication is a consideration for moderate to severe endo patients. An example of this is Orilissa. It’s marketed as a non-hormonal form of treatment that’s been clinically proven to reduce painful periods, pelvic pain in between periods, and pain with sex. Side effects are the same as the above GnRH agonists.
Pelvic floor physiotherapy has also been gaining a lot more traction for endometriosis pain treatment. Your pelvic floor is a network of muscles that steady the pelvis, support the organs of the pelvis, and stabilize connected joints like the hip and sacroiliac joint. Chronic disease like endometriosis can cause dysfunction of these muscles, but pelvic floor physical therapy an help relieve a lot of the symptoms associated with endo.
The only true end to endometriosis is by way of a hysterectomy (aka surgical removal of the lady parts). For most women of childbearing age living with endometriosis, a hysterectomy is not first-line treatment due to the fact that they often wanna have babies before taking out their uterus. This surgical procedure is irreversible, therefore if the patient knows they no longer want to have children, this would be the means to which they could get rid of their endometriosis once a for all.
If you have endometriosis, feel free to reach out to me and share your story with this diagnosis. You can comment below, email me, or find me on social. There is strength in numbers!









Leave a comment